If you’ve noticed your breasts sitting lower than they used to, looking emptier at the top, or feeling heavier and less perky, you’re not alone. “Saggy breasts” (the medical term is breast ptosis) are incredibly common and a completely normal part of life. Ageing, pregnancy, weight changes and genetics all play a role. The good news is there are effective, evidence-based treatments—from supportive measures to surgical lifts—that can restore shape, position and confidence.
We explain what really causes sagging, how our surgeons assess it, what genuinely helps (and what doesn’t), and the safest, most reliable treatments available at Deansgate Hospital for patients across Manchester, Liverpool, Cheshire and the North West.
Key Takeaways
-
Sagging is natural and relates to skin elasticity, breast tissue composition and the position/strength of the breast’s support system.
-
Creams, “miracle” supplements and exercises don’t lift sagging breast tissue; they may improve skin quality or posture, but they cannot elevate the nipple or tighten stretched skin.
-
The only definitive way to lift the breast and reposition the nipple is mastopexy (breast lift) surgery—with or without adding volume using implants or your own fat.
-
Choosing the right technique (lift alone, lift with implants, auto-augmentation, fat transfer) depends on your degree of ptosis, skin quality, desired size/shape, and future plans (pregnancy/weight change).
-
An experienced, FRCS(Plast) consultant plastic surgeon will customise a plan that prioritises safety, shape longevity and natural aesthetics.
What Do We Mean by “Saggy Breasts”?
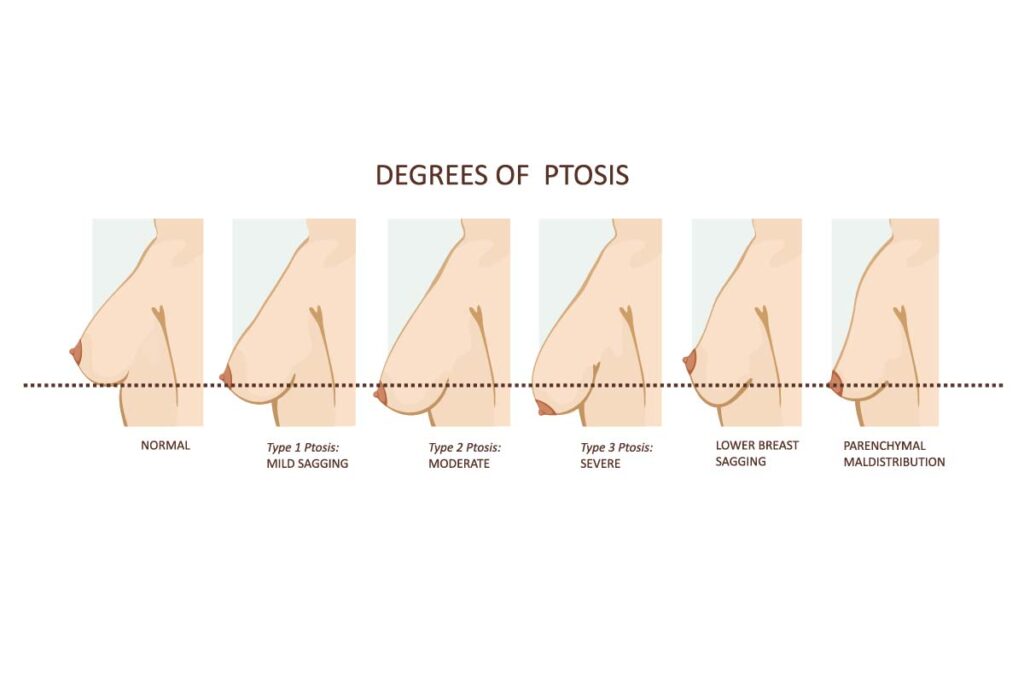
Breast ptosis describes the downward descent of the breast mound and the nipple-areola complex relative to the breast fold (inframammary fold, IMF). Classically, surgeons use Regnault’s grading:
-
Grade I (Mild): Nipple is at the level of the IMF.
-
Grade II (Moderate): Nipple is below the IMF but still above the lowest point of the breast.
-
Grade III (Severe): Nipple is the lowest point of the breast, pointing downward.
-
Pseudoptosis: The nipple sits at/above the fold, but most tissue hangs below it (often seen after weight loss or post-pregnancy).
-
Parenchymal maldistribution / bottoming-out: Tissue migrates inferiorly over time, sometimes after previous augmentation if the pocket or support isn’t ideal.
This grading guides the type of lift and whether augmentation (implants or fat) is likely to be beneficial.
Why Do Breasts Sag?
1) Ageing and Collagen Loss
Skin loses collagen and elastin with age, reducing recoil. The internal breast ligaments (Cooper’s ligaments) lengthen, and the envelope becomes lax.
2) Pregnancy and Breastfeeding
Breasts often enlarge during pregnancy, stretching the skin. After pregnancy/breastfeeding, glandular tissue may involute (shrink), leaving a looser envelope with less internal “fill”—the classic deflated upper pole look. This is a key driver of post-pregnancy ptosis, irrespective of whether you breastfeed.
3) Weight Changes
Breasts contain a variable mix of glandular and fatty tissue. Significant weight loss reduces fatty volume, frequently creating pseudoptosis (fullness at the bottom, emptier top).
4) Genetics and Natural Anatomy
Your skin type, ligament strength, breast size/weight, and chest wall shape are partly genetic. Heavier breasts are more prone to descent over time due to gravity.
5) Smoking
Smoking impairs microcirculation and collagen synthesis, reducing skin quality and healing capacity.
6) Poorly Fitting Bras
A supportive bra won’t “treat” ptosis, but consistent poor support—especially during high-impact activity—can contribute to discomfort and progressive stretching.
Myths vs Facts
-
Myth: “Push-ups and chest exercises will lift my breasts.”
Fact: Exercise strengthens pectoralis muscles under the breast but doesn’t tighten breast skin or ligaments. It can improve chest contour and posture, which helps appearance, but it does not elevate the nipple.
-
Myth: “Topical creams can lift the breast.”
Fact: Some active skincare may improve skin texture and hydration; nothing topical can reposition tissue relative to the IMF.
-
Myth: “Breastfeeding causes sagging.”
Fact: Pregnancy itself (volume fluctuation and skin stretch) is the main factor; breastfeeding is not the sole culprit.
-
Myth: “Implants always fix sagging.”
Fact: Implants add volume. If the nipple is below the fold, you usually need a lift (mastopexy) with or without an implant. An implant alone can worsen bottoming-out in a ptotic breast.
How We Assess Saggy Breasts at Deansgate Hospital
Your consultation is a consultant plastic surgeon, bespoke assessment:
-
History & Goals
-
Weight stability, pregnancy plans, breast symptoms (rashes under fold, bra-strap grooves), previous surgery.
-
Desired size, upper-pole fullness, and cleavage preferences.
-
-
Examination
-
Nipple position vs IMF (Regnault grade).
-
Skin quality, stretch marks, asymmetry, areola size, chest wall shape.
-
Breast composition (gland vs fat) and ptosis pattern (true ptosis vs pseudoptosis).
-
-
Options & Planning
-
Lift alone vs lift + implant vs auto-augmentation (using your own tissue) vs fat transfer.
-
Incision pattern appropriate to the degree of ptosis.
-
Safety planning, recovery and realistic longevity.
-
Non-Surgical Options: What Helps (and What Doesn’t)
-
Supportive bras: Improve comfort, posture and silhouette. Sports bras for activity; professionally fitted everyday bras can be transformative in clothes.
-
Weight stability: Avoid significant fluctuations; stable weight helps preserve results after surgery.
-
Skin health: Sun protection; avoid smoking; consider medical-grade skincare for texture and firmness (not lift).
-
Physio/posture training: Can subtly enhance upper-chest contour and how breasts sit visually on the thorax.
Bottom line: Non-surgical measures do not reverse established ptosis but can improve appearance and comfort.
Surgical Treatments for Saggy Breasts
1) Mastopexy (Breast Lift)
What it does: Breast lift removes excess skin, reshapes the breast mound, and elevates the nipple to a youthful, central position. It also allows areola resizing if enlarged.
Common incision patterns (chosen to match your ptosis grade and goals):
-
Periareolar (Benelli / “donut”): Scar around the areola. Useful for mild lifts and areola reduction. Limited vertical lift; not for severe ptosis.
-
Vertical (Lollipop): Around the areola + a vertical line to the IMF. Excellent shaping, useful for mild–moderate ptosis, often the workhorse technique.
-
Wise-pattern (Anchor): Around the areola + vertical + along the IMF. Best for moderate–severe ptosis, significant reshaping or when there’s substantial excess skin.
Pros:
-
Definitive repositioning of the nipple and tightening of the envelope.
-
Improves shape, projection and symmetry.
Considerations:
-
Scars are permanent but usually fade well.
-
Doesn’t add volume—upper-pole fullness can be improved with internal reshaping, but if you want a fuller look, consider implant or fat transfer.
2) Mastopexy with Implants (Augmentation Mastopexy)
Who it suits: If you want a lift and more volume, especially upper-pole fullness and cleavage.
How it works: A breast lift is combined with a carefully selected implant. The sequence (single-stage vs staged procedures) is personalised to minimise risks such as wound tension or implant malposition.
Pros:
-
Rejuvenates position and increases size/upper-pole fullness.
-
Can address deflation after pregnancy/weight loss.
Considerations:
-
Slightly higher complexity than either procedure alone; meticulous pocket control is vital to avoid bottoming-out.
-
Implants are medical devices; you’ll discuss implant type, profile, placement (subfascial, dual-plane) and long-term surveillance.
3) Auto-Augmentation Mastopexy
Who it suits: Patients who want more upper-pole fullness without a foreign body (implant). The surgeon rearranges your own lower-pole tissue to auto-augment the upper pole during the lift.
Pros:
-
Natural tissue; improved upper-pole without implant.
-
Elegant option in selected anatomies, especially with pseudoptosis.
Considerations:
-
Doesn’t create as large an increase in size as an implant.
-
Requires excellent surgical planning to maintain long-term support.
4) Fat Transfer (Lipofilling) to the Breast
What it is: Your own fat is harvested (e.g., from abdomen/flanks), processed, and injected into the breast to improve contour and subtle volume.
Pros:
-
Natural and soft; can enhance upper-pole and correct minor asymmetry.
-
Useful adjunct to a lift; can be repeated.
Considerations:
-
Limited volume per session; some fat is reabsorbed (expect ~50–70% retention).
-
Not a substitute for a lift when nipples are low; often combined with mastopexy.
Choosing the Right Approach: A Quick Guide
-
Mild ptosis, happy with size: Mastopexy (periareolar or vertical).
-
Moderate/severe ptosis, happy with size: Vertical or Wise-pattern mastopexy.
-
Ptosis + want fuller, rounder look: Augmentation-mastopexy (implant) or auto-augmentation +/- fat transfer.
-
Deflation with pseudoptosis, minimal lift needed: Auto-augmentation or fat transfer (if nipple is at/above IMF).
-
Post-pregnancy, “empty” upper pole: Lift + implant or auto-augmentation +/- fat transfer, depending on size goals and tissue quality.
At consultation in Manchester, we’ll discuss outcomes, review before/after cases and match techniques to your anatomy and goals.
Safety, Risks and Recovery
All surgery carries risks. At Deansgate Hospital you’ll have a thorough consent process, focusing on safety first.
General risks:
-
Bruising, swelling, infection, delayed healing.
-
Sensation changes (often temporary), particularly around the areola.
-
Scarring: initially red/raised, softens and fades over 6–12 months; scar care is provided.
Mastopexy-specific:
-
Asymmetry, residual/relapse of ptosis with time (gravity and ageing continue).
-
Widening scars in patients with poor skin quality or significant tension.
With implants:
-
Capsular contracture, implant malposition, rippling, rupture (over the long term).
-
The need for future revision at some stage in life.
With fat transfer:
-
Partial fat resorption, oil cysts, calcifications (usually benign and distinguishable on imaging).
Recovery timeline (typical):
-
Home the same day or overnight depending on case.
-
Supportive bra for 6 weeks.
-
Desk work in 7–10 days; driving ~1–2 weeks once comfortable.
-
Gym/impact exercise 4–6 weeks; heavier lifting 6–8 weeks (surgeon-specific).
-
Swelling improves over 8–12 weeks; scars mature over months.
We provide enhanced recovery protocols, scar care guidance (e.g., silicone therapy), and structured follow-up.
Longevity of Results
A breast lift turns back the clock but doesn’t stop it. Results typically remain pleasing for years. Longevity is best with:
-
Stable weight and a supportive bra.
-
Avoidance of smoking and excessive sun exposure.
-
Realistic expectations regarding future pregnancies and ageing.
If you plan pregnancy soon, you might prefer to delay mastopexy until after your family is complete to maximise durability.
Can I Get a Lift Without Visible Scars?
Any meaningful lift requires skin removal, which means scars. The art is placing scars where they are least conspicuous, achieving superior shape, and supporting excellent healing with modern closure techniques and scar care. Most patients find scars a worthwhile trade-off for the rejuvenated shape and comfort.
Will a Lift Affect Breastfeeding or Sensation?
Modern techniques preserve as much glandular tissue and blood supply as possible. Breastfeeding after mastopexy may still be possible, but cannot be guaranteed. Nipple sensation often recovers over time; a small proportion of patients may experience persistent changes (reduced or, less commonly, hypersensitivity). Our surgeon will explain risks based on your anatomy and chosen technique.
Costs and Financing
Costs vary by technique, complexity, and whether implants or fat transfer are added. After your consultation and individualised surgical plan, you’ll receive a clear, all-inclusive quotation. We can also discuss available finance options and scheduling at Deansgate Hospital.
Why Choose Deansgate Hospital for Saggy Breasts?
-
Consultant-led care: Experienced FRCS(Plast) surgeons with a strong aesthetic focus.
-
Bespoke planning: We listen to your goals and tailor your technique accordingly.
-
Safety culture: CQC-aligned standards, robust pre-op assessment and aftercare.
-
Natural results: Shape, proportion and long-term support are prioritised.
-
Comprehensive options: Lift alone, lift with implants, auto-augmentation, and fat transfer.
Whether you’re seeking a subtle perk-up or a full mummy makeover, our team designs a plan around your body, your lifestyle and your vision.
FAQs About Saggy Breasts
Do bras prevent sagging?
A well-fitted bra doesn’t reverse ptosis but supports the breast, improves comfort, and may slow progressive stretching in heavy breasts—especially during exercise.
Can I fix sagging without surgery?
You can improve the appearance with bras, posture and skin care, but meaningful lift requires surgery.
Will implants alone lift my breasts?
Only if your nipples are already at/above the IMF and you simply want more volume. If nipples are low, an implant alone may make the breast heavier and worsen ptosis; a lift is usually needed.
How long do results last?
Many years, especially with stable weight and good support. Ageing continues, and mild settling over time is normal.
What about future pregnancy?
Pregnancy may change breast volume and skin again. If you plan children soon, you may prefer to delay surgery for durability.
Is a breast lift painful?
Most patients describe discomfort rather than severe pain. We use modern anaesthesia and enhanced recovery to keep you comfortable.
Will I have scars?
Yes, but they fade with time and careful scar care. Your surgeon will choose the most appropriate pattern to balance lift and scar minimisation.
What’s the difference between a lift and auto-augmentation?
A lift removes skin and repositions tissue; auto-augmentation additionally re-arranges your own tissue to enhance upper-pole fullness—ideal if you don’t want an implant.
Next Steps
Book a personal consultation at Deansgate Hospital in Manchester to discuss your goals, body, and lifestyle. We’ll examine your anatomy, review options, show you typical results, and design a treatment plan that delivers natural, long-lasting improvement with the highest safety standards.



